Cranioplasty: how the integrity of the skull is restored after serious injuries
Cranioplasty is the surgical repair of defects in the cranial vault
(the dome-shaped part of the skull). It sounds complicated, but in
reality, it is an operation that closes the “hole” in the head
caused by trauma or disease. Why is this necessary? First, the brain
needs to be protected from mechanical damage. Second, an intact skull
helps fluids circulate properly around the brain. Third, it is
important for the patient's appearance and psychological comfort.
(the dome-shaped part of the skull). It sounds complicated, but in
reality, it is an operation that closes the “hole” in the head
caused by trauma or disease. Why is this necessary? First, the brain
needs to be protected from mechanical damage. Second, an intact skull
helps fluids circulate properly around the brain. Third, it is
important for the patient's appearance and psychological comfort.
When is cranioplasty
necessary?
necessary?
Skull defects can
occur in several ways:
occur in several ways:
After severe head
injuries. In cases of serious fractures, when the bone is shattered,
surgeons have to remove the damaged fragments to prevent them from
entering the brain.
injuries. In cases of serious fractures, when the bone is shattered,
surgeons have to remove the damaged fragments to prevent them from
entering the brain.
In cases of critical
brain edema. When the brain swells sharply due to a stroke,
hemorrhage, or severe trauma, doctors perform a decompressive
craniectomy — removing part of the bone to give the brain room to
expand and save the patient's life. Later, when the swelling
subsides, this bone must be put back in place.
brain edema. When the brain swells sharply due to a stroke,
hemorrhage, or severe trauma, doctors perform a decompressive
craniectomy — removing part of the bone to give the brain room to
expand and save the patient's life. Later, when the swelling
subsides, this bone must be put back in place.
Due to infection.
Sometimes an infection of the bone tissue (osteomyelitis) develops in
the area of the operation, and the infected area of the bone has to
be removed.
Sometimes an infection of the bone tissue (osteomyelitis) develops in
the area of the operation, and the infected area of the bone has to
be removed.
For tumors. If a
tumor affects the skull bone, surgeons remove that area along with
the tumor and then restore the brain's protection.
tumor affects the skull bone, surgeons remove that area along with
the tumor and then restore the brain's protection.
Trepanation
syndrome: when the defect affects life
syndrome: when the defect affects life
After removing part
of the skull, patients often develop an unpleasant condition that
doctors call trepanation syndrome. Imagine: a hollow forms in the
head, and the skin above it sinks inward. Atmospheric pressure
literally presses on the brain through this hollow.
of the skull, patients often develop an unpleasant condition that
doctors call trepanation syndrome. Imagine: a hollow forms in the
head, and the skin above it sinks inward. Atmospheric pressure
literally presses on the brain through this hollow.
How it feels:
-- Headache —
often worse when standing or sitting. The pain is less severe when
lying down because atmospheric pressure is less intense.
often worse when standing or sitting. The pain is less severe when
lying down because atmospheric pressure is less intense.
-- Dizziness and
fatigue — patients feel exhausted and have difficulty
concentrating.
fatigue — patients feel exhausted and have difficulty
concentrating.
-- Memory and
thinking problems — the person has trouble remembering information,
finds it difficult to plan, and becomes distracted.
thinking problems — the person has trouble remembering information,
finds it difficult to plan, and becomes distracted.
-- Sensory
disturbances or weakness in the legs and arms, speech problems.
disturbances or weakness in the legs and arms, speech problems.
-- Unexpected
seizures (epileptic seizures) — new to the patient or worsening of
old ones.
seizures (epileptic seizures) — new to the patient or worsening of
old ones.
-- Heart and blood
pressure problems — a sharp drop in blood pressure when standing up
(orthostatic hypotension).
pressure problems — a sharp drop in blood pressure when standing up
(orthostatic hypotension).
This condition
significantly impairs quality of life: the person cannot work
normally, is afraid to go outside, cannot play sports, or lie in a
position where their head is higher than their heart.
significantly impairs quality of life: the person cannot work
normally, is afraid to go outside, cannot play sports, or lie in a
position where their head is higher than their heart.
What materials are
used for reconstruction
used for reconstruction
When a surgeon
reconstructs a defect, they may use:
reconstructs a defect, they may use:
The patient's own
bone
bone
If the removed bone
was preserved (frozen or placed under the skin) during the first
operation, it can be returned to its place.
was preserved (frozen or placed under the skin) during the first
operation, it can be returned to its place.
Pros: This is
“native” material, it is a perfect fit, and the body does not
reject it.
“native” material, it is a perfect fit, and the body does not
reject it.
Cons: Unfortunately,
the patient's own bone often becomes thinner or even dissolves in the
body (especially in young people or if a drainage system is installed
in the brain). In addition, there is a risk of infection. As a
result, in about 20-40% of cases, this bone has to be removed again
and replaced with something else.
the patient's own bone often becomes thinner or even dissolves in the
body (especially in young people or if a drainage system is installed
in the brain). In addition, there is a risk of infection. As a
result, in about 20-40% of cases, this bone has to be removed again
and replaced with something else.
Titanium plates
A durable metal used
to make custom plates that are precisely tailored to the shape of the
patient's defect (based on their CT scans).
to make custom plates that are precisely tailored to the shape of the
patient's defect (based on their CT scans).
Pros: Titanium is
very resistant to infection, lasts a long time, and looks good.
People who are active and afraid of getting hit on the head can rest
assured that titanium will hold up.
very resistant to infection, lasts a long time, and looks good.
People who are active and afraid of getting hit on the head can rest
assured that titanium will hold up.
Cons: There may be
slight interference with MRI and CT scans. Standard titanium mesh
(not customized) can cause steps and shift, so it is better to order
a customized 3D plate.
slight interference with MRI and CT scans. Standard titanium mesh
(not customized) can cause steps and shift, so it is better to order
a customized 3D plate.
PEEK (high-tech
polymer)
polymer)
A modern material
that is also used to make customized plates based on CT scans.
that is also used to make customized plates based on CT scans.
Pros: Its properties
are very similar to those of real bone. Minimal complications, good
cosmetic results, no interference with MRI, and good acceptance by
the body.
are very similar to those of real bone. Minimal complications, good
cosmetic results, no interference with MRI, and good acceptance by
the body.
Cons: Expensive. It
takes time to manufacture using special technologies (CAD/CAM). Not
available everywhere.
takes time to manufacture using special technologies (CAD/CAM). Not
available everywhere.
PMMA (acrylic
cement)
cement)
A substance that can
be shaped directly during surgery.
be shaped directly during surgery.
Pros: Cheap, fast,
the surgeon can adjust the shape directly during the operation.
the surgeon can adjust the shape directly during the operation.
Cons: Emits heat
when hardening (needs to be cooled). More prone to infection, may
crack over time, especially if the defect is large. According to
statistics, infection develops in approximately 14% of cases.
when hardening (needs to be cooled). More prone to infection, may
crack over time, especially if the defect is large. According to
statistics, infection develops in approximately 14% of cases.
“Reperen”
(Russian polymer material)
(Russian polymer material)
Plates made of a
specially synthesized polymer that become soft and easily moldable
when heated in hot water.
specially synthesized polymer that become soft and easily moldable
when heated in hot water.
Pros: Well
compatible with the body, tissues grow into the holes in the plate
and create a strong bond. Clearly visible on MRI and CT scans. More
affordable than PEEK, more convenient than PMMA. Domestic development
with good local results.
compatible with the body, tissues grow into the holes in the plate
and create a strong bond. Clearly visible on MRI and CT scans. More
affordable than PEEK, more convenient than PMMA. Domestic development
with good local results.
Cons: Less
international data on long-term results. For very complex or large
defects, more expensive PEEK or custom titanium is often recommended.
international data on long-term results. For very complex or large
defects, more expensive PEEK or custom titanium is often recommended.
Calcium phosphate
materials (hydroxyapatite)
materials (hydroxyapatite)
Ceramics that mimic
the mineral part of the bone and gradually fuse with the real bone.
the mineral part of the bone and gradually fuse with the real bone.
Pros: The body
treats the material as its own, and osseointegration (ingrowth)
occurs. Good cosmetic result.
treats the material as its own, and osseointegration (ingrowth)
occurs. Good cosmetic result.
Cons: More fragile
than other options, may break upon impact. Requires some caution and
protection in the early stages.
than other options, may break upon impact. Requires some caution and
protection in the early stages.
When to perform
cranioplasty: optimal timing
cranioplasty: optimal timing
If part of the skull
has been removed, when is the best time to restore its integrity?
Based on current research, doctors recommend:
has been removed, when is the best time to restore its integrity?
Based on current research, doctors recommend:
The optimal time is
within the first 2-3 months after bone removal, if the patient's
condition allows.
within the first 2-3 months after bone removal, if the patient's
condition allows.
Why is it better to
do it sooner?
do it sooner?
-- Neurological
deficits recover faster (in 40-75% of cases, memory, thinking, and
mobility improve).
deficits recover faster (in 40-75% of cases, memory, thinking, and
mobility improve).
-- The risk of
chronic problems with fluid circulation in the brain is reduced.
chronic problems with fluid circulation in the brain is reduced.
-- Normal
relationships between the brain and skull are better restored, and
blood supply improves.
relationships between the brain and skull are better restored, and
blood supply improves.
But you can't rush
if:
if:
-- The brain is
still very swollen and may prolapse (bulge) into the hole that has
formed — in this case, closing the defect is dangerous.
still very swollen and may prolapse (bulge) into the hole that has
formed — in this case, closing the defect is dangerous.
-- The patient has
an active infection (meningitis, wound infection).
an active infection (meningitis, wound infection).
-- There are
problems with cerebrospinal fluid circulation (hydrocephalus), and a
drainage system must first be installed.
problems with cerebrospinal fluid circulation (hydrocephalus), and a
drainage system must first be installed.
What complications
can occur
can occur
Unfortunately, even
after a well-performed cranioplasty, approximately 18-36% of patients
experience some problems.
after a well-performed cranioplasty, approximately 18-36% of patients
experience some problems.
Infectious
complications (suppuration, osteomyelitis) — wound infection or
infection of the implant itself. This may require removal of the
material. The risk is higher with autogenous bone and PMMA, lower
with titanium and PEEK.
complications (suppuration, osteomyelitis) — wound infection or
infection of the implant itself. This may require removal of the
material. The risk is higher with autogenous bone and PMMA, lower
with titanium and PEEK.
Resorption of
autogenous bone — if autogenous bone was used, it may thin or
dissolve completely in 20-50% of cases. In this case, repeat surgery
is required.
autogenous bone — if autogenous bone was used, it may thin or
dissolve completely in 20-50% of cases. In this case, repeat surgery
is required.
Mechanical problems
— displacement or fracture of the implant, incorrect shape, which
is especially noticeable in the face and forehead area.
— displacement or fracture of the implant, incorrect shape, which
is especially noticeable in the face and forehead area.
Wound problems —
necrosis of the skin edges, suture separation, fluid accumulation
(seromas and hematomas). In some cases, this occurs in 30% of
patients.
necrosis of the skin edges, suture separation, fluid accumulation
(seromas and hematomas). In some cases, this occurs in 30% of
patients.
Problems with fluid
in the brain — cerebrospinal fluid pressure changes, a hernia may
develop in the defect, air may appear in the skull (pneumocerebellar
syndrome).
in the brain — cerebrospinal fluid pressure changes, a hernia may
develop in the defect, air may appear in the skull (pneumocerebellar
syndrome).
New seizures —
approximately 8-15% of patients experience epileptic seizures, which
can usually be controlled with medication.
approximately 8-15% of patients experience epileptic seizures, which
can usually be controlled with medication.
Systemic
complications — bleeding, blood clots, reactions to anesthesia.
complications — bleeding, blood clots, reactions to anesthesia.
How to choose the
material for a specific patient
material for a specific patient
The choice depends
on several factors:
on several factors:
If long-term
reliability and low risk of repeat operations are critical → choose
PEEK or custom titanium. Yes, it is more expensive, but statistically
there are fewer problems.
reliability and low risk of repeat operations are critical → choose
PEEK or custom titanium. Yes, it is more expensive, but statistically
there are fewer problems.
If the defect is
medium to large and the budget is limited → custom titanium offers
a good balance of price and quality.
medium to large and the budget is limited → custom titanium offers
a good balance of price and quality.
If the defect is
small, there is no history of infection, and it can be modeled
directly during surgery → PMMA or “Reperen” is possible.
small, there is no history of infection, and it can be modeled
directly during surgery → PMMA or “Reperen” is possible.
If the patient has
already had problems with infections or has a system installed in the
brain → avoid PMMA and their own bone, choose titanium, PEEK, or
hydroxyapatite.
already had problems with infections or has a system installed in the
brain → avoid PMMA and their own bone, choose titanium, PEEK, or
hydroxyapatite.
If the operation is
needed quickly and it is impossible to wait for the plate to be
manufactured → PMMA or ready-made plates must be chosen.
needed quickly and it is impossible to wait for the plate to be
manufactured → PMMA or ready-made plates must be chosen.
What the patient
needs to know
needs to know
Cranioplasty is a
serious but modern operation. With the right choice of material and
compliance with all conditions (no infection, stable brain condition,
qualified surgeon), it gives good results.
serious but modern operation. With the right choice of material and
compliance with all conditions (no infection, stable brain condition,
qualified surgeon), it gives good results.
Many patients report
a reduction in headaches, improved memory and concentration, and a
return of self-confidence after the procedure.
a reduction in headaches, improved memory and concentration, and a
return of self-confidence after the procedure.
The risk of
complications is real, but it is reduced by performing the surgery in
a timely manner (within the first 2-3 months), choosing modern
materials, and proper preparation.
complications is real, but it is reduced by performing the surgery in
a timely manner (within the first 2-3 months), choosing modern
materials, and proper preparation.

Plastic surgery of the defect of the frontal bone with a mesh plate made of reperene.

Plastic surgery of the defect of the frontal bone with a mesh plate made of reperene.

Fixation of a fragment of the frontal bone with a titanium plate.

Plastic surgery of the skull defect in the sagittal sinus area with a titanium plate.

Fixation of frontal bone fragments in severe TBI with titanium plates.

Manufacturing of an individual implant made of acrylic cement based on a model of the patient's skull, made on the basis of preoperative MSCT of the brain.

Manufacturing of an individual implant made of acrylic cement based on a model of the patient's skull before surgery and reconstruction of the skull based on MSCT of the patient's brain after surgery.

Plastic surgery of the anterior wall of the frontal sinus with a mesh titanium plate.

Plastic surgery of the frontal bone defect with an individual mesh titanium plate made on the basis of preoperative MSCT of the brain.
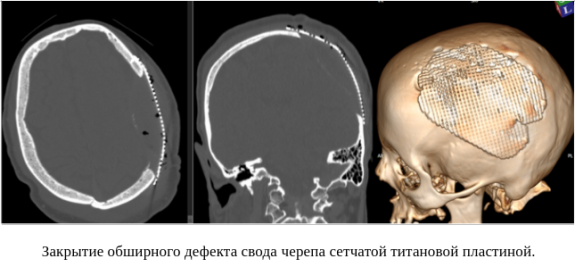
Closure of an extensive defect in the cranial vault with a mesh titanium plate.

Due to bone flap resorption, a titanium mesh plate was used to close the bone defect.

Deformation of the titanium mesh plate due to impact during a domestic fight.